GENEMEDICS APP
GENEMEDICS NUTRITION
Potential Benefits of Aminophylline
Aminophylline offers various health benefits, including weight loss promotion, enhanced cognitive function, improved sleep quality, better cardiovascular health, treatment of lung diseases and injuries, as well as enhanced kidney function.
- Promotes weight loss [1-13]
- Improves cognitive function [14-26]
- Improves sleep quality [27-33]
- Improves cardiovascular health [34-52]
- Treats lung diseases/injuries [53-93]
- Improves kidney function [94-129]
Key Takeaways of Aminophylline
- Aminophylline is commonly used as a bronchodilator to treat respiratory conditions like asthma and chronic obstructive pulmonary disease (COPD). It relaxes the airway muscles, making it easier to breathe.
- Aminophylline therapy requires careful dosing and monitoring of serum theophylline concentrations to maintain therapeutic levels and avoid toxicity. Adjustments to the dose may be necessary based on an individual’s response and potential side effects.
- Aminophylline acts more rapidly than theophylline, making it suitable for situations requiring quick relief from bronchospasms or respiratory distress.
- Like any medication, aminophylline can cause side effects, including nausea, vomiting, nervousness, and cardiac arrhythmias (changes in heart rhythm). Patients should be monitored for adverse reactions during treatment.
- Beyond its role as a bronchodilator, aminophylline may have potential applications in specific medical conditions, such as improving cardiovascular performance in COPD patients or treating central sleep apneas. Always consult with a healthcare professional for accurate dosing and guidance.
What is Aminophylline?
Aminophylline is known as a potent bronchodilator medicine. This means that it opens the airways of the lungs by relaxing the smooth muscles. Because of this effect, aminophylline is prescribed for the treatment of wheezing, breathing difficulties, asthma, emphysema, chronic bronchitis, acute bronchospasm, and other respiratory disorders.
Aminophylline Mechanism of Action
Aminophylline inhibits the enzyme phosphodiesterase-4 (PDE-4) which is found in cells of the lungs. PDE-4 inhibition increases the levels of intracellular cyclic adenosine monophosphate (cAMP) in target cells. This process results in the following effects:
- Relaxation of the smooth muscles of the lungs to allow more air in
- Reduction of inflammation by decreasing the sensitivity of the lungs to allergens
- Increased contractions of the diaphragm
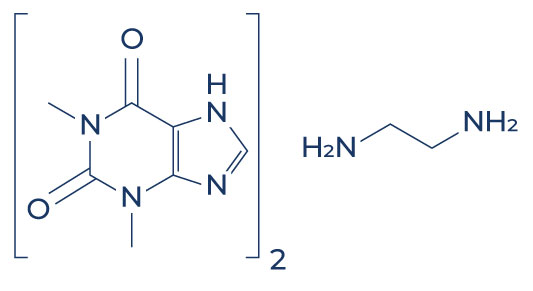
Chemical Structure of Aminophylline
Research on Aminophylline
Promotes Weight Loss

A good deal of evidence suggests that aminophylline can improve body composition by reducing body fat percentage and promoting lean muscle mass:
- In overweight men and women, the application of 0.5% aminophylline cream to the waist twice a day was associated with a significant reduction in waist circumference. [1]
- In participants with fat deposits on their thighs, the application of aminophylline lotion significantly reduced thigh circumference, thigh skinfold thickness, and thigh fat mass. [2]
- Twelve weeks of 0.5% aminophylline cream administration significantly decreased waist-to-hip ratios in overweight female participants compared to male participants. [3]
- A study found that aminophylline promotes fat loss by inducing the breakdown of fat cells. [4]
- In women with lower body fat distribution, the application of aminophylline cream significantly reduced thigh fat. [5]
- In overweight women, the application of 10% aminophylline ointment to the thigh five times a week for 6 weeks with diet and walking resulted in significant girth loss from the treated thigh. [6]
- In sedentary females, the application of a cream containing aminophylline, caffeine, yohimbe, l-carnitine, and gotu kola twice daily for 28 days was more effective at reducing thigh circumference, thigh skinfold thickness, and thigh fat mass compared to a placebo combined with a walking program and a restricted caloric intake. [7]
- In patients with cellulite (persistent subcutaneous fat causing dimpling of the skin), the application of aminophylline cream resulted in fat reduction and improvements in the texture of the skin. [8-10]
- A review of data from two small clinical trials showed that the use of aminophylline cream was associated with reduced thigh girth with no adverse effects. [11]
- In obese women who were placed on a calorie-restricted diet, the application of aminophylline cream resulted in significant girth loss compared with a placebo injection or cream. [12]
In female subjects, the application of aminophylline cream to areas with unwanted body fat for 6 weeks caused a significant reduction in subcutaneous fat and girth. [13]
Improves Cognitive Function
 Studies also support that aminophylline has cognitive-boosting properties, making it beneficial in a broad range of conditions affecting brain function:
Studies also support that aminophylline has cognitive-boosting properties, making it beneficial in a broad range of conditions affecting brain function:
- The administration of escalating doses of aminophylline in patients who received sevoflurane anesthesia accelerated postoperative cognitive recovery. [14-16]
- In school-aged patients, aminophylline administration led to greater improvement on all tests of memory and concentration. [17]
- In patients with brain damage, aminophylline administration improved cognitive function by increasing oxygen levels within the brain. [18]
- In healthy, male, moderate drinkers, treatment with aminophylline (200 mg) significantly reduced ethanol’s effects on the electroencephalogram (EEG) and motor coordination. [19]
- In rats exposed to restrain stress, aminophylline (4mg/kg) modulated the stress in a significant manner. [20]
- In patients anesthetized with total intravenous anesthesia, the administration of aminophylline at 4 mg/kg shortened cognitive recovery time. [21]
- In rats exposed to low oxygen levels, immediate administration of aminophylline significantly improved long-term neurobehavioral achievements. [22]
- In patients who received isoflurane anesthesia, the administration of high doses of aminophylline expedited the extubation (tube removal) time and was associated with improved recovery of vigilance and neuromotor functions. [23-24]
- In patients who received halothane, a general anesthesia, the administration of aminophylline accelerated cognitive recovery. [25]
- In patients who received total intravenous anesthesia (TIVA) with propofol and remifentanil, aminophylline 3 mg/kg shortened the time to spontaneous ventilation and improved early recovery without adverse side effects. [26]
Improves Sleep Quality

Aminophylline administration can also help treat sleeping difficulties associated with various medical conditions:
- In healthy male volunteers, aminophylline administration normalized high-altitude sleep-disordered breathing. [27]
- In patients with obstructive sleep apnea syndrome (a condition in which the walls of the throat interrupt normal breathing during sleep), aminophylline improved impaired breathing and increased NREM (non-rapid eye movement) sleep or dreamless sleep. [28]
- In patients with sleeping difficulties related to acute mountain sickness, aminophylline administration improved sleep efficiency without any adverse effects. [29]
- In a patient with severe, predominantly central sleep apnea (a potentially serious sleep disorder in which breathing repeatedly stops and starts) due to damage to the medulla, the bottom-most part of the brain, aminophylline administration improved respiration at the onset of sleep. [30]
- In thiopental-anesthetized rats, aminophylline improved sleep times and transmission of nerve signals in the brain. [31]
- In mature infants with sleep apnea syndrome, aminophylline treatment for 1 week significantly reduced apneas (breathing repeatedly stops and starts) and cyanosis (bluish skin discoloration) during sleep. [32-33]
Improves Cardiovascular Health

There’s also increasing evidence showing that aminophylline can help improve heart health:
- A study found that aminophylline has the ability to restore normal heart rhythm, thus reducing the risk of heart failure and other fatal heart conditions. [34]
- In chronic obstructive pulmonary disease (COPD) patients, oral and intravenous administration of aminophylline enhanced both right and left heart systolic pump function. [35-36]
- In human subjects, aminophylline administration increased heart rate and cardiac output via stimulation of the sympathetic nervous system. [37-38]
- In COPD patients, aminophylline administration improved global cardiac function and reduced dyspnea (difficulty in breathing). [39-40]
- In animal models, aminophylline improved left ventricular contractility and heart rate variability (interval between heartbeats). [41-42]
- In patients with an occluded heart artery, intravenous aminophylline infusion at 5 mg/kg over 20 minutes significantly delayed the time to onset of exercise-induced ischemia (insufficient blood flow) and improved blood circulation. [43]
- In patients with congenital or acquired heart disease, aminophylline caused a decrease in arterial pressure, left ventricular pressure, right and left atrial pressure, total systemic resistance, and total pulmonary resistance. [44]
- In patients with cardiac failure due to hypertension or coronary heart disease, aminophylline produced consistent and significant increases in cardiac output while decreasing heart pressure. [45]
- In patients with acute inferior myocardial infarction treated with aspirin and streptokinase (a medication that dissolves blood clots), the addition of intravenous aminophylline reversed abnormal heart rhythm. [46]
- In patients with cardiac arrest who do not respond to the standard treatment, the administration of aminophylline (rapid intravenous injection of 250 mg) established a stable heart rhythm with sufficient blood pressure. [47]
- In rabbit hearts, small doses of aminophylline increased the rate and amplitude of heart contractions. [48]
- In patients with angina (chest pain due to reduced blood flow to the heart muscle), a reduction in the total number of episodes of chest pain was reported by the subjects after 6 weeks of aminophylline treatment. [49]
- In patients with severe cases of bradycardia (abnormally low heart rate) who do not respond to the standard treatment, intravenous aminophylline eliminated the need for pacemaker placement. [50]
- In patients with symptomatic bradycardia due to spinal cord injury, the addition of aminophylline to the therapeutic regimen was associated with the resolution of the bradycardia. [51]
- In patients with valvular heart disease, aminophylline increased blood circulation to the heart and lungs by inducing vasodilation (widening of the blood vessels). [52]
Treats Lung Diseases/Injuries

Aminophylline is often prescribed for a multitude of lung conditions. There’s robust evidence supporting the benefits of this drug on pulmonary health:
- In adults hospitalized for acute asthma, treatment with aminophylline was associated with fewer nebulizations of albuterol and a lower rate of exacerbations (worsening of symptoms). [53-54]
- In patients with acute severe asthma, aminophylline infusions improved lung function and symptoms. [55]
- In patients with respiratory fatigue, aminophylline administration reduced the risk of intubation. [56]
- In patients with partially reversible severe airway obstruction, intravenous injection of aminophylline (250 mg) was associated with consistent improvement in the mean forced expiratory volume, a measure of how much air a person can exhale during a forced breath. [57]
- In patients with acute exacerbation of asthma or chronic obstructive pulmonary disease, aminophylline infusion decreased hospital admissions. [58]
- In patients with chronic obstructive pulmonary disease (COPD), aminophylline administration improved symptoms by reducing the levels of inflammatory markers. [59]
- In patients with COPD, oral administration of aminophylline (400 mg) increased mean forced expiratory volume and forced vital capacity. [60-61]
- In patients with COPD, low-dose aminophylline increased the efficacy of inhaled corticosteroids by reducing the incidence of exacerbations. [62-63]
- In patients undergoing valve replacement, aminophylline administration had an anti-inflammatory effect and improved pulmonary oxygenation. [64]
- The prolonged use of maintenance aminophylline therapy in COPD patients increased diaphragmatic contractility and endurance and improved several aspects of mucociliary function (defense mechanism of the lungs). [65]
- The administration of long-acting 225-mg aminophylline compounds twice daily for 8 weeks improved the peak expiratory flow rate in younger COPD patients and relieved symptoms of chest tightness in older COPD patients. [66]
- Aminophylline administration in COPD patients enhanced the anti-inflammatory effect of corticosteroids. [67]
- In patients with chronic bronchitis and moderate to severe chronic obstruction to airflow, aminophylline administration at 800 mg daily led to an improvement in peripheral ventilation. [68]
- In normal young adults, aminophylline prevented alterations in breathing patterns. [69]
- In patients with mild asthma, low-dose aminophylline led to a significant reduction in mean sputum eosinophils (a measure of allergic reaction). [70]
- In patients with atopic asthma, aminophylline administration at 200 mg every 12 hours reduced airway inflammatory response to allergen inhalation. [71]
- In patients with right-sided heart failure due to COPD, aminophylline produced a significant reduction in mean pulmonary artery pressure and increased alveolar ventilation (a process by which oxygen is brought into the lungs). [72]
- In chronic asthmatic patients with regular nocturnal exacerbations who took 450 mg slow-release aminophylline at midnight, a significant increase in mean peak expiratory flow rates (a measure of air flowing out of the lungs) was observed. [73]
- In animal models, aminophylline administration improved survival by enhancing lung maturation. [74-79]
- In animal models of meconium aspiration syndrome, a condition in which a newborn breathes in a mixture of meconium (the earliest stool of an infant) and amniotic fluid into the lungs, aminophylline treatment enhanced lung functions and alleviated oxidative injury and changes in airway reactivity related to lung inflammation. [80-82]
- In mice, the administration of aminophylline (20/kg twice daily) attenuated lung scarring by decreasing collagen production. [83]
- In healthy subjects, aminophylline significantly improved the contractile function of the exhausted human diaphragm, rendering it less susceptible to fatigue. [84-86]
- In rabbits with pulmonary edema (lung inflammation) due to acid injury, aminophylline prevented the increase in lung weight and pulmonary artery pressure. [87-88]
- A study found that high doses of aminophylline may diminish inflammatory recruitment of neutrophils to the lungs, thus reducing injury. [89]
- In children over two years receiving inhaled bronchodilators, aminophylline treatment resulted in greater improvement in lung function compared with placebo. [90]
- A cell study found that aminophylline protected lung cells against programmed cell death (apoptosis) induced by cigarette smoking. [91]
- In premature infants, the administration of aminophylline reduced the risk of chronic lung disease and respiratory distress. [92-93]
Improves Kidney Function

Numerous studies also support the beneficial effects of aminophylline on kidney function and related diseases:
- In patients with acute kidney injury, aminophylline therapy significantly improved renal excretory function as evidenced by increased urine output. [94]
- In neonates and children, a single dose of aminophylline prevented acute kidney injury and severe renal dysfunction. [95]
- In patients with renal colic, a type of pain associated with kidney stones, the administration of 375 mg of aminophylline reduced pain by 24% to 39%. [96]
- Aminophylline administration also reduced the prevalence of acute kidney injury after cardiac surgery in pediatric patients. [97]
- In patients with acute renal failure, aminophylline administration was associated with an improvement in renal function indices. [98]
- In premature infants, aminophylline improved kidney function by enhancing urinary calcium and uric acid excretion. [99]
- Intravenous aminophylline administration in human subjects was associated with a 52% reduction in the risk of contrast-induced acute kidney injury. [100-101]
- In intensive care unit patients with acute kidney injury, aminophylline infusion at 5 mg/kg increased urine output. [102]
- In patients admitted to a general intensive care unit following major surgery, aminophylline administration increased blood flow to the kidneys and improved the glomerular filtration rate (filtering ability of the kidneys). [103]
- In patients undergoing chemotherapy, aminophylline administration prevented the deterioration of the glomerular filtration rate. [104]
- In patients with contrast-induced acute renal failure after coronary angioplasty, the administration of aminophylline countered the harmful effects of the contrast on the kidneys. [105]
- In patients with stones in the urethra, aminophylline reduced stone migration to the kidneys. [106]
- In mice with renal ischemia (insufficient blood flow to the kidneys), aminophylline administration at 5 mg/kg improved renal function and indexes of kidney inflammation. [107]
- In pediatric patients with acute kidney injury, aminophylline administration improved kidney function by increasing urine output and preventing complications. [108-110]
- In pediatric patients who had heart surgery, the administration of aminophylline prevented acute kidney injury and resulted in a significant increase in urine output. [111-116]
- In neonates with low oxygen levels, aminophylline use was associated with an increase in urine output and improvement in the glomerular filtration rate. [117-120]
- In patients who had coronary angiography, a procedure that uses contrast to visualize how blood flows through your heart on an X-ray screen, aminophylline prevented contrast-induced kidney deterioration. [121]
- In patients with liver cirrhosis (liver damage due to scarring), the administration of aminophylline at 3 mg/kg increased free-water production. [122]
- In rats with vancomycin-induced acute kidney injury, the administration of aminophylline at a dose of 24 mg/kg once daily significantly reduced the elevations in kidney enzymes. [123]
- In rats with acute kidney failure caused by the chemotherapeutic drug cisplatin, aminophylline administration at 24 mg/kg every 12 hours alleviated kidney dysfunction. [124]
- In patients with severe chronic kidney disease (CKD), aminophylline significantly reduced the prevalence of gastrointestinal adverse effects associated with traditional treatment for CKD. [125-126]
- In patients with acute kidney injury, aminophylline improved urine flow rate (UFR) and reduced the need for dialysis. [127]
- In high-risk patients, the use of aminophylline infusion was associated with a lower incidence of deterioration in kidney function following heart surgery. [128-129]
Aminophylline Uses

Aminophylline, known by the aminophylline brand name “Phyllocontin” among others, is a bronchodilator that is used to treat and prevent the symptoms of asthma, bronchitis, chronic obstructive pulmonary disease (COPD), and other lung conditions. It’s essential to be aware of different brand names, as they can vary depending on the region or country. Always consult with a healthcare professional when seeking information about specific medications.
The following are aminophylline indications:
Asthma
Aminophylline is used to treat acute exacerbations of asthma and can help prevent asthma attacks by relaxing the muscles around the airways.

COPD (Chronic Obstructive Pulmonary Disease)
Chronic obstructive pulmonary disease, which includes conditions like chronic bronchitis and emphysema, can also be managed with aminophylline. It helps reduce breathlessness and wheezing in these patients.

Bronchitis
This drug helps in alleviating the symptoms of bronchitis by opening the bronchial airways, facilitating better airflow.
Apnea in Premature Infants
Aminophylline can be used to stimulate breathing in premature infants who suffer from apnea (periods when breathing stops).

Diagnostic Testing
Sometimes, aminophylline is used as part of diagnostic tests for certain respiratory conditions, such as asthma and other chronic lung diseases, because of its ability to open up the airways.
Aminophylline works by relaxing and opening air passages in the lungs, making it easier to breathe. The drug is a combination of theophylline and ethylenediamine. It’s essential to monitor theophylline blood levels when using aminophylline, as the therapeutic range is narrow, and there’s a risk of side effects if levels become too high. Always use aminophylline as directed by a healthcare professional to manage conditions like asthma and other chronic lung diseases effectively.
Aminophylline Contraindications
Aminophylline is a medication that is used to treat certain respiratory conditions, such as asthma and chronic obstructive pulmonary disease (COPD). However, there are several contraindications or situations in which aminophylline should not be used. These contraindications include:
Hypersensitivity
Aminophylline should not be used in individuals who have a known hypersensitivity or allergy to aminophylline, theophylline, or other xanthine derivatives.
Active Peptic Ulcer Disease
Aminophylline can increase gastric acid secretion, which may exacerbate symptoms and worsen peptic ulcer disease. It should be avoided in individuals with active peptic ulcers.
Seizure Disorders
Aminophylline can lower the seizure threshold, making seizures more likely to occur. It should be used with caution in individuals with underlying seizure disorders.
Cardiac Arrhythmias
Aminophylline can lead to cardiac arrhythmias, especially in high doses, which may result in an increased risk of severe heart rhythm disturbances. Therefore, it should be avoided or used with extreme caution in individuals with pre-existing arrhythmias, as they may be at an increased risk of experiencing these potentially dangerous side effects.
Congestive Heart Failure
Aminophylline may exacerbate congestive heart failure symptoms. It should be used cautiously, if at all, in individuals with heart failure.
Liver Disease
Individuals with severe liver disease or hepatic dysfunction may have impaired clearance of aminophylline from the body, leading to higher blood levels and an increased risk of toxicity. This is because the liver plays a crucial role in metabolizing and eliminating aminophylline. In cases of hepatic dysfunction, the liver’s ability to perform these metabolic processes may be compromised. As a result, the drug may accumulate in the bloodstream, potentially causing adverse effects such as nausea, vomiting, cardiac arrhythmias, and seizures. Healthcare providers should exercise caution when prescribing aminophylline to individuals with hepatic dysfunction and consider dose reduction or alternative treatments to minimize the risk of toxicity. Regular monitoring of serum theophylline concentrations is essential in such cases to ensure that a safe and effective dose is maintained.
Active Gastrointestinal Bleeding
Aminophylline can irritate the gastrointestinal tract and increase the risk of bleeding. It should not be used in cases of active gastrointestinal bleeding.
Thyroid Disorders
Aminophylline may affect thyroid hormone levels. It should be used with caution in individuals with thyroid disorders.
Children and Elderly
Special caution should be exercised when using aminophylline in children and the elderly, as they may be more sensitive to its effects.
Pregnancy and Breastfeeding
Aminophylline should be used during pregnancy or breastfeeding only if the potential benefits outweigh the risks, and under the supervision of a healthcare provider. It’s essential to discuss your medical history and any pre-existing conditions with your healthcare provider before starting aminophylline or any new medication to ensure it is safe and appropriate for your specific situation. During breastfeeding, aminophylline may pass into breast milk, potentially affecting the nursing infant. Therefore, your healthcare provider should carefully consider the necessity of aminophylline treatment while breastfeeding and monitor both the mother and baby for any adverse effects.
Associated Side Effects of Aminophylline
Aminophylline side effects are very uncommon. There have been some side effects associated with the use of this drug wherein the patient had one of the issues listed below at some point while being on aminophylline. However, these side effects weren’t confirmed to be associated with the treatment and could have been a coincidence and not related to the use of aminophylline. Despite this, it was listed as a side effect associated with aminophylline even though these associated side effects are very uncommon.
Side effects associated with aminophylline may include the following:
- Allergic skin reaction
- Changes in heartbeat and heart rhythm
- Elevated liver enzymes
- Headache
- Heartburn
- Increase in urine volume
- Increased gastric acid secretion
- Insomnia
- Irritability
- Nausea
- Restlessness
- Shakiness
- Vomiting
- Yellow skin and eyes
Aminophylline Dosage
The dosage of aminophylline can vary depending on the specific medical condition being treated, the patient’s age, weight, and overall health, as well as the formulation of the medication (oral, intravenous, etc.). In general, aminophylline dosage in mcg/mL is typically between 10 and 20 mcg/mL. This is the therapeutic range, meaning that this is the range of concentrations that is most likely to be effective in treating asthma and other respiratory conditions without causing side effects. It is crucial to follow the prescribing healthcare provider’s instructions and the dosing information provided on the medication label or packaging. Typically, aminophylline is administered as an injection or oral tablet.
For the treatment of acute bronchospasm in adults, the usual recommended intravenous dosage is an initial loading dose of 5-6 mg/kg of aminophylline infused over 20-30 minutes, followed by a continuous intravenous infusion at a rate of 0.4-0.9 mg/kg/hour to maintain therapeutic levels. The total daily dose should not typically exceed 800 mg unless specifically directed by a healthcare provider. Adjustments in the maintenance dose may be necessary based on the patient’s response to ensure they receive therapeutic doses of the medication.
For children, the dosage may be different and should be determined by a healthcare provider based on the child’s weight and condition. The use of divided doses may be considered to achieve the desired therapeutic effect while minimizing side effects. Dose reduction may also be a consideration if the patient experiences adverse reactions or if serum theophylline concentrations exceed the therapeutic range.
It’s important to note that aminophylline therapy often requires careful monitoring of blood levels (serum theophylline concentrations) to avoid toxicity. Dosing adjustments, including both dose reduction and modification of the maintenance dose, may be necessary based on the patient’s response and any potential side effects. Always consult a healthcare professional or physician for the most accurate and appropriate dosage adjustments for your specific medical situation.
Aminophylline vs Theophylline
Aminophylline and theophylline are both medications that belong to a class of drugs called methylxanthines. While they have some similarities, they also have distinct differences:
Chemical Composition
Aminophylline: Aminophylline is a compound composed of theophylline and ethylenediamine. It is a water-soluble derivative of theophylline.
Theophylline: Theophylline is a naturally occurring compound and is the primary active component of aminophylline. When theophylline is administered intravenously, it can lead to increased serum theophylline levels due to its rapid absorption into the bloodstream. This increased theophylline concentration can be particularly concerning in patients with decreased theophylline clearance, such as those with liver or kidney impairment, as they are at a higher risk of experiencing toxic effects.
Medical Uses
Aminophylline: Aminophylline is typically used in emergency situations and acute care settings, such as in the treatment of severe asthma attacks or chronic obstructive pulmonary disease (COPD) exacerbations. Its administration aims to rapidly achieve therapeutic serum concentrations to address the acute respiratory distress seen in these conditions. Monitoring serum concentrations is essential to ensure appropriate drug dosing and effectiveness during the treatment process.
Theophylline: Theophylline is used for the long-term management and prevention of asthma and COPD symptoms. It is taken regularly to maintain stable respiratory function. Regular monitoring of theophylline clearance is essential in patients receiving theophylline therapy to ensure that serum theophylline levels remain within the therapeutic range. Elevated serum theophylline levels can lead to adverse effects, including nausea, vomiting, cardiac arrhythmias, and seizures. Healthcare providers must adjust theophylline dosage based on the patient’s individual theophylline clearance rate to optimize therapeutic benefits while minimizing the risk of toxicity.
While theophylline itself is not a histone deacetylase activator (a substance that helps control how genes work in our cells by modifying the structure of proteins called histones), it plays a crucial role in managing respiratory conditions by modulating bronchial smooth muscle tone and inflammation, which are essential factors in asthma and COPD management.
It’s important for healthcare professionals to recognize that factors such as age, smoking status, and concurrent medication use can also influence theophylline clearance. Therefore, individualized dosing and vigilant monitoring of serum theophylline levels are crucial to providing safe and effective theophylline therapy for patients with respiratory conditions like asthma or chronic obstructive pulmonary disease (COPD).
Administration
Aminophylline: Aminophylline injection is often administered intravenously (IV) or intramuscularly (IM) in acute situations where a rapid response is needed. Serum concentrations of aminophylline injection are closely monitored during administration to ensure the desired therapeutic effect and to prevent adverse reactions. It is essential for healthcare providers to maintain appropriate serum concentrations of aminophylline injection to achieve the desired clinical outcomes. Proper monitoring of aminophylline injection levels allows healthcare professionals to adjust the dose as needed for optimal patient care.
Theophylline: Serum theophylline concentrations are usually monitored closely in patients taking theophylline to ensure its therapeutic levels are maintained. Theophylline is usually taken orally in the form of tablets, capsules, or extended-release preparations. It is designed for chronic use and provides a sustained effect. Serum theophylline concentrations are usually monitored closely in patients taking theophylline to ensure its therapeutic levels are maintained.
Onset of Action
Aminophylline: Aminophylline acts more rapidly than theophylline, making it suitable for situations requiring quick relief, such as acute bronchospasms. This rapid onset of action is due to the fact that aminophylline injection rapidly undergoes metabolic conversion within the body, leading to the release of theophylline, which then exerts its bronchodilatory effects. Understanding theophylline metabolism is essential in this context, as the conversion of aminophylline injection to theophylline increases its bioavailability and therapeutic efficacy. Theophylline metabolism is influenced by factors such as liver function, age, genetics, and drug interactions, which can affect the rate at which aminophylline injection is converted to the active theophylline compound. Therefore, healthcare providers must consider these factors when determining the appropriate use of aminophylline injection in clinical practice.
Theophylline: Theophylline has a slower onset of action and is used for maintenance therapy to prevent respiratory symptoms over an extended period. Monitoring serum theophylline concentrations is essential to ensure therapeutic efficacy and prevent toxicity. Regular assessment of serum theophylline concentration allows healthcare providers to adjust dosage regimens as needed, ensuring that patients maintain optimal drug levels for effective management of their respiratory conditions. Additionally, healthcare professionals can use serum theophylline concentration measurements to identify and address any potential signs of theophylline overdose or toxicity in a timely manner, promoting patient safety during the course of treatment.
It’s important to note that theophylline distributes poorly into tissues with high-fat content, which can affect its pharmacokinetics. Factors such as age, liver function, and concurrent use of other medications can also influence theophylline clearance. Healthcare providers may consider dose adjustments or therapeutic drug monitoring to increase theophylline clearance in patients with altered pharmacokinetics. Utilizing anhydrous theophylline formulations can also play a role in maintaining consistent drug levels and optimizing therapeutic outcomes, as these formulations offer precise dosing options and can contribute to better control of serum theophylline concentration.
Half-Life
Aminophylline: Aminophylline has a shorter half-life compared to theophylline. The difference in half-life can be attributed to the fact that aminophylline injection consists of theophylline and ethylenediamine, which is rapidly converted into theophylline in the body. This conversion process contributes to the faster onset of action and shorter duration of effect observed with aminophylline injection.
It’s important to note that aminophylline clearance is influenced by various factors, including genetics, liver function, and drug interactions. Additionally, theophylline administered to individuals with certain medical conditions may result in altered metabolism rates. Understanding these nuances in theophylline metabolism is crucial for healthcare providers to optimize drug therapy and minimize the risk of adverse effects.
Theophylline: Serum theophylline concentrations are routinely monitored in patients receiving theophylline therapy to ensure therapeutic levels are maintained. Theophylline clearance varies among individuals, and regular monitoring of serum theophylline concentrations helps healthcare providers adjust dosage regimens to achieve optimal therapeutic levels while minimizing the risk of toxicity. This careful management of serum theophylline concentrations is essential for the safe and effective treatment of conditions such as asthma or chronic obstructive pulmonary disease (COPD).
Theophylline metabolism can be influenced by various factors, including age, liver function, and concurrent medications. Healthcare providers need to be vigilant in monitoring serum theophylline concentrations and theophylline metabolism in patients with these considerations. It’s crucial to assess how theophylline is being metabolized in an individual patient and whether the dosage regimen needs modification.
In some cases, anhydrous theophylline formulations may be preferred, as they offer precise dosing options and can contribute to better control of serum theophylline concentrations. These formulations can be particularly beneficial when fine-tuning theophylline therapy in patients with varying clearance rates. By closely monitoring theophylline clearance and utilizing appropriate formulations, healthcare providers can optimize treatment outcomes while ensuring patient safety.
Dosage Monitoring
Aminophylline: Aminophylline levels, specifically serum concentrations, are usually monitored closely in emergency situations to avoid toxicity. Regular monitoring of serum concentrations ensures that aminophylline clearance remains within the therapeutic range (commonly measured in mcg/ml) and helps prevent adverse effects. Healthcare providers use these serum concentration measurements to make informed decisions about dosage adjustment or the need for additional interventions to maintain aminophylline levels within safe and effective limits, typically within the recommended therapeutic range. Monitoring also allows healthcare professionals to tailor the treatment to the patient’s specific needs, ensuring the best possible outcome in emergency situations where aminophylline is administered.
Theophylline: Serum theophylline concentrations are monitored regularly in chronic therapy to ensure that therapeutic levels are maintained and to prevent toxicity. Monitoring serum theophylline concentrations, which reflect theophylline clearance, is crucial for adjusting dosage regimens and optimizing the management of individuals receiving theophylline therapy. It allows healthcare providers to fine-tune treatment to achieve the desired therapeutic effect while avoiding potentially harmful levels of the drug in the bloodstream.
Additionally, healthcare providers use serum theophylline concentrations, a key indicator of theophylline clearance, to make informed decisions regarding dose adjustments and to minimize the risk of adverse effects associated with theophylline therapy. Monitoring theophylline clearance is an essential part of ensuring the safe and effective use of this medication. Your healthcare provider will adjust dose as per clinical needs.
Side Effects and Safety
Both aminophylline and theophylline can have side effects, including nausea, vomiting, nervousness, and cardiac arrhythmias. However, aminophylline may have a higher risk of adverse effects due to its more rapid action. Additionally, monitoring serum concentrations of both drugs is essential to ensure that they remain within the therapeutic range and do not lead to toxic effects.
The term “narrow therapeutic index” refers to medications that have a small margin of safety between their minimum effective dose and the minimum toxic dose. In other words, drugs with a narrow therapeutic index have a small window between the dose that provides a therapeutic effect and the dose that can lead to harmful or toxic effects. For such medications, it is crucial to maintain drug levels within this narrow range to achieve the desired therapeutic outcome while avoiding harmful side effects.
In the context of aminophylline and theophylline, both drugs fall under the category of medications with a narrow therapeutic index. This means that maintaining the serum concentrations of these drugs within a specific range is essential to ensure their effectiveness and safety. Deviating from this narrow range can lead to adverse effects, including nausea, vomiting, nervousness, and cardiac arrhythmias. Aminophylline, in particular, carries a higher risk of adverse effects due to its more rapid action.
Therefore, it is imperative for healthcare providers to regularly monitor serum theophylline concentrations when prescribing these drugs. By doing so, they can make informed decisions about dose adjustments, if necessary, to keep the drug levels within the therapeutic range. This monitoring helps optimize the therapeutic benefits of aminophylline and theophylline while minimizing the potential for toxic effects, ensuring the safe and effective management of various medical conditions.
Regularly assessing serum theophylline concentration is also crucial to maintaining optimal drug levels and minimizing the risk of side effects. Healthcare providers should closely monitor these levels to make necessary adjustments in the treatment regimen if needed, ensuring the safety and effectiveness of theophylline therapy.
Availability
Aminophylline: Aminophylline is typically administered in healthcare settings by healthcare professionals. The dosage and administration of aminophylline are carefully monitored to maintain appropriate serum concentrations within the therapeutic range, typically measured in mcg/ml, ensuring the desired clinical effects while minimizing the risk of adverse reactions. This close monitoring of serum concentrations helps healthcare providers make informed decisions regarding dosage adjustments and the overall management of aminophylline therapy for the patient’s specific medical condition.
Theophylline: Theophylline is available in various oral formulations and is prescribed for home use under medical supervision. However, in certain clinical situations where rapid onset of action is required, intravenous theophylline may be administered. It’s important to note that the rate of absorption and onset of action of intravenous theophylline differs significantly from oral theophylline.
When theophylline is administered intravenously, it undergoes rapid absorption into the bloodstream, leading to an immediate increase in serum theophylline levels. This rapid increase can be advantageous in situations where prompt therapeutic effects are needed, such as in the management of acute exacerbations of respiratory conditions like asthma.
On the other hand, oral theophylline typically has a slower onset of action, as it must first be absorbed from the gastrointestinal tract before entering the bloodstream. While it can provide long-term maintenance therapy for chronic respiratory conditions, it may not be suitable for rapidly addressing acute symptoms.
Healthcare providers must carefully consider the appropriate route of administration and dosage when prescribing theophylline to patients based on their clinical presentation and treatment goals. Close monitoring of theophylline levels is crucial, as both intravenous and oral theophylline increases carry the potential for adverse effects if serum concentrations exceed the therapeutic range.
In summary, while aminophylline and theophylline are related medications with similar therapeutic effects, they are used in different clinical scenarios and have variations in administration, onset of action, and safety profiles. The choice between them depends on the specific medical condition and the required treatment approach. Patients should always follow their healthcare provider’s recommendations regarding the use of these medications.
Aminophylline Before and After
About Dr. George Shanlikian
Dr. George Shanlikian, renowned as the world’s best hormone therapy doctor, possesses expertise in various medical domains. These include Bio-Identical Hormone Replacement Therapy, Peptide Replacement Therapy, Anti-Aging Medicine, Regenerative Medicine, Stress Management, Nutrition Consulting, Nutritional Supplement Consulting, and Exercise Consulting.
Read more about him here: https://www.genemedics.com/dr-george-shanlikian-md-best-hormone-therapy-doctor
Read more success stories here:
Men’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/mens-success-stories/
Women’s Success Stories: https://www.genemedics.com/about-ghi/ghi-success-stories/womens-success-stories/
FAQ
What should I check before giving aminophylline?
Before giving aminophylline, you should check the patient’s medical history, including any history of hypersensitivity to the drug, pre-existing medical conditions such as heart or liver disease, current medications, and drug interactions. Additionally, it’s essential to assess the potential transfer of aminophylline into breast milk if the patient is a breastfeeding mother, as this could impact a nursing infant. Patients with a history of acute hepatitis should be closely monitored when prescribed aminophylline, as liver function may be compromised, potentially affecting drug metabolism and clearance. It’s essential to consider these factors to ensure the safe and effective administration of aminophylline in clinical practice.
What are the precautions for aminophylline?
Precautions for aminophylline include monitoring for signs of toxicity, especially in patients with a history of aminophylline sensitivity or underlying medical conditions. Aminophylline should be used with caution in patients with heart arrhythmias, seizures, hyperthyroidism, and gastrointestinal disorders, as these conditions may increase the risk of adverse effects, given its narrow therapeutic index.
Careful monitoring of serum theophylline levels is essential to prevent overdose and maintain aminophylline within the appropriate therapeutic range, considering its narrow therapeutic index. Patients with hepatic impairment may metabolize aminophylline differently, potentially leading to altered drug levels, so close monitoring is essential. Additionally, aminophylline can affect renal function, and patients with renal impairment should be closely monitored for any signs of metabolic acidosis or changes in renal function. Irregular heartbeat is a potential side effect of aminophylline, and healthcare providers should closely monitor cardiac function during treatment to detect any signs of irregular heartbeat and take appropriate measures if needed.
For breastfeeding mothers, it’s important to note that aminophylline can pass into breast milk, potentially affecting nursing infants. Healthcare providers should carefully weigh the benefits of aminophylline treatment against the potential risks to the infant, and mothers may need to consider alternative feeding options while undergoing aminophylline therapy. Similarly, pregnant individuals should discuss the potential risks and benefits of aminophylline treatment with their healthcare provider, as the drug may affect the developing fetus.
How often to take aminophylline?
The frequency of aminophylline administration depends on the specific medical condition being treated and the healthcare provider’s prescription. It can be administered as a single dose, multiple doses per day, or as an intravenous infusion. For chronic lung conditions like asthma or chronic obstructive pulmonary disease (COPD), aminophylline is often prescribed as a maintenance therapy, typically with multiple doses per day to ensure a sustained bronchodilatory effect and improved respiratory function.
Dosage adjustment may be necessary based on the patient’s response to treatment and any potential side effects, ensuring that the therapy remains effective and safe over time. Monitoring of serum aminophylline levels, typically measured in mcg/ml, is important in maintaining therapeutic concentrations and avoiding toxicity. Healthcare providers use these measurements to make informed decisions about dosing regimens and to ensure that patients receive the appropriate amount of aminophylline for their specific medical conditions.
When is the best time to take aminophylline?
The timing of aminophylline administration can vary depending on the condition. It is best to follow the healthcare provider’s instructions for the specific dosing schedule. Monitoring the timing of aminophylline administration is crucial to ensure that peak serum concentrations are achieved when needed for the desired therapeutic effect. This timing may be especially important in acute situations where rapid bronchodilation or relief from respiratory distress is required, as achieving peak serum concentrations promptly can help maximize the drug’s effectiveness.
Aminophylline is available in various forms, including oral tablets and an oral solution. The choice of formulation may also influence the timing of administration, as oral solutions may be absorbed more rapidly than tablets, potentially leading to a faster onset of action.
Can aminophylline be taken without food?
Aminophylline is available in various forms, including oral tablets, intravenous injections, and oral solutions. When administering the oral solution, patients should follow the prescribed dosing schedule for consistency. Monitoring the serum concentration of aminophylline is crucial to determine if adjustments in dosage are needed to achieve therapeutic levels and avoid toxicity. This close monitoring helps healthcare providers make informed decisions about the medication’s effectiveness and safety for the patient, regardless of the formulation used.
Why should aminophylline be given slowly?
Aminophylline should be given slowly to minimize the risk of adverse effects and toxicity, particularly in patients with renal impairment, as their ability to clear the drug from the body may be compromised. Rapid administration can lead to serious side effects and should be avoided. Monitoring serum concentration levels is essential during the administration of aminophylline to ensure that the drug remains within the therapeutic range and to prevent any potential complications. Healthcare providers use these serum concentration measurements, typically expressed in mcg/ml, to make informed decisions about dosage adjustments or the need for additional interventions to maintain aminophylline levels within safe and effective limits. Proper dosing and monitoring are crucial to achieving the desired therapeutic outcomes while minimizing the risk of adverse reactions.
Does aminophylline need to be protected from light?
Yes, aminophylline should be protected from light to prevent degradation of the drug. Exposure to light can lead to chemical changes in aminophylline, which may affect its stability and efficacy. It’s essential to store aminophylline in a container that shields it from direct light to maintain the desired serum concentration and therapeutic effects. Proper storage conditions help ensure that the medication remains effective and safe for use. Always follow the recommended storage instructions provided with the specific formulation of aminophylline you are using to maintain its serum concentration within the therapeutic range.
What drugs should not be taken with aminophylline?
Several drugs should not be administered concomitantly with aminophylline, including other xanthine derivatives (xanthine drugs) like theophylline or caffeine, as these substances can potentially impact the central nervous system and serum concentrations of aminophylline, leading to a range of adverse effects. The consideration of potential drug interactions is crucial when prescribing or using aminophylline, as taking it with certain medications can result in a harmful drug combination, affecting its therapeutic effects and safety profile. Healthcare providers must carefully evaluate a patient’s medication regimen to minimize the risk of adverse reactions and ensure the most effective treatment.
To safeguard patient health, it is imperative to provide a comprehensive list of all medications, including vitamin supplements, in use to the healthcare provider. This enables the assessment of potential drug interactions, ensuring that serum concentrations of aminophylline remain within the therapeutic range, thereby promoting safe and effective treatment. Monitoring serum concentration levels is a crucial step in managing these interactions and optimizing patient care, especially considering the potential impact on the central nervous system.
How does aminophylline affect heart rate?
Aminophylline may affect heart rate by increasing it in some cases, especially when administered rapidly, and this effect can be more pronounced in elderly patients due to age-related changes in cardiac function. Such patients may experience a more significant heart rate increase when given aminophylline. Monitoring heart rate is essential during aminophylline therapy in elderly patients to ensure their safety and adjust the dosage if necessary. Additionally, healthcare providers should consider the overall health and medical history of such patients when determining the appropriate use of aminophylline to minimize potential cardiac-related side effects, especially if they have a history of cardiac disease.
What are the desired effects of aminophylline?
The desired effects of aminophylline include bronchodilation, improved airflow, increased oxygen exchange, and relief from symptoms of respiratory distress, such as wheezing and shortness of breath. Aminophylline is commonly used in the management of chronic lung diseases, where it helps alleviate symptoms and improve lung function. Its bronchodilatory properties make it particularly beneficial for individuals with conditions like asthma and chronic obstructive pulmonary disease (COPD). Aminophylline achieves these effects by relaxing the smooth muscle cells lining the airways, reducing constriction, and allowing for easier airflow.
By relaxing airway smooth muscles, aminophylline facilitates easier breathing and enhances overall respiratory function in patients with chronic lung diseases. However, it’s important to note that aminophylline has a narrow therapeutic index, meaning that the difference between a therapeutic dose and a potentially toxic dose is small. Therefore, careful monitoring of serum theophylline concentrations is essential to ensure that patients remain within the safe and effective therapeutic range, minimizing the risk of adverse effects.
Does aminophylline increase respiratory rate?
Aminophylline may increase respiratory rate in some cases, primarily by improving bronchial airflow and oxygenation.
Does aminophylline affect sleep?
Aminophylline can affect sleep in some individuals, potentially causing insomnia or restlessness as a side effect.
Can aminophylline cause tachycardia?
Aminophylline can cause tachycardia (increased heart rate) as a side effect, especially when administered rapidly. This cardiac stimulation is often observed due to aminophylline’s bronchodilatory effects and its impact on adenosine receptors, which can increase heart rate. It is essential for healthcare providers to monitor patients closely when administering aminophylline to detect and manage any cardiovascular side effects promptly. Adjustments to the dosage or infusion rate may be necessary to mitigate the risk of excessive cardiac stimulation and maintain patient safety during treatment.
Does aminophylline cause bradycardia?
Aminophylline is not typically associated with bradycardia (slow heart rate) as a side effect.
Can salbutamol and aminophylline be taken together?
Salbutamol and aminophylline can be taken together in some cases, but the combination should be carefully monitored and prescribed by a healthcare provider. Combining these medications may help achieve better bronchodilation and improved respiratory function in individuals with severe asthma or other respiratory conditions. However, it’s essential to be aware of potential adverse reactions that can arise when using both medications concurrently.
Regular check-ups and close supervision by a healthcare provider are crucial to assess the effectiveness of the combination therapy while minimizing the risk of adverse reactions. Adjustments to the dosages may be necessary based on the patient’s response and the presence of any side effects associated with the combined use of salbutamol and aminophylline.
How does aminophylline help respiratory distress syndrome?
Aminophylline can help treat respiratory distress syndrome by improving bronchial airflow and oxygenation and reducing symptoms of airway constriction, thereby preventing respiratory failure. Monitoring for higher serum concentrations of aminophylline is essential during treatment to ensure that therapeutic levels are maintained and potential side effects are minimized. This careful monitoring plays a critical role in managing respiratory distress syndrome and optimizing patient outcomes.
Is aminophylline used in heart failure?
Aminophylline may be used in heart failure cases under specific circumstances, but it should be prescribed and monitored by a healthcare provider to minimize the risk of cardiovascular complications.
Can aminophylline be given with normal saline?
Aminophylline can be given with normal saline, depending on the patient’s condition and the healthcare provider’s recommendations.
How long to continue aminophylline infusion?
The duration of aminophylline infusion varies based on the patient’s condition and the healthcare provider’s prescription.
How long does aminophylline stay in your system?
Aminophylline can stay in the system for several hours to days, with the exact duration varying among individuals.
Can aminophylline be inhaled?
Aminophylline can be administered via inhalation in some cases, typically using a nebulizer, to treat specific respiratory conditions.
Why is aminophylline important in pulmonary edema?
Aminophylline is important in pulmonary edema because it helps improve bronchial airflow and oxygenation, which can be critical in managing the condition.
What effects does aminophylline have on potassium?
Aminophylline can affect potassium levels in the body, potentially leading to hypokalemia (low potassium levels) as a side effect.
How does aminophylline prevent apnea?
Aminophylline can help prevent apnea in premature infants by stimulating respiratory drive and improving lung function.
Is aminophylline a diuretic?
Aminophylline is not typically considered a diuretic, as its primary function is to improve bronchial function and respiratory symptoms.
What is the use of aminophylline in cardiac?
Aminophylline may be used in cardiac cases to improve bronchial airflow and oxygenation, especially in cases where respiratory distress is a concern.
Does aminophylline cause hyperglycemia?
Aminophylline can sometimes cause hyperglycemia (high blood sugar) as a side effect.
Can aminophylline be used with a nebulizer?
Aminophylline can be used with a nebulizer in specific respiratory conditions, but the administration method should be determined by a healthcare provider.
Which is better aminophylline or salbutamol?
The choice between aminophylline and salbutamol depends on the specific medical condition and the healthcare provider’s prescription.
How does aminophylline affect the kidneys?
Aminophylline may affect kidney function in some cases, potentially leading to changes in urine output. Monitoring kidney function is important during aminophylline therapy to detect any abnormalities or signs of serious toxicity related to kidney function. This monitoring involves regular assessments of urine output, renal function tests, and overall renal health. Healthcare providers closely watch for any signs of kidney dysfunction, such as decreased urine output, elevated creatinine levels, or changes in electrolyte balance, to ensure the safe and effective use of aminophylline in patients.
How does aminophylline affect urine output?
Aminophylline can affect urine output, and changes in urine output should be monitored during treatment.
Can I take Ventolin and aminophylline together?
Ventolin and aminophylline can be taken together in some cases, but the combination should be prescribed and monitored by a healthcare provider.
How do you give aminophylline for asthma?
The administration of aminophylline for asthma varies depending on the specific asthma management plan and should be prescribed and monitored by a healthcare provider. The recommended dosage of aminophylline is typically based on the patient’s weight and is often expressed in micrograms per milliliter (mcg/ml) to ensure precise dosing. It’s crucial for healthcare providers to calculate the appropriate dosage and monitor serum concentrations of aminophylline (mcg/ml) regularly to maintain therapeutic levels and prevent potential side effects or toxicity. This personalized approach helps ensure that patients receive the most effective and safe treatment for their asthma.
Reference
Caruso MK, Pekarovic S, Raum WJ, Greenway F. Topical fat reduction from the waist. Diabetes ObesMetab. 2007;9(3):300-3.
Escalante G, Bryan P, Rodriguez J. Effects of a topical lotion containing aminophylline, caffeine, yohimbe, l-carnitine, and gotu kola on thigh circumference, skinfold thickness, and fat mass in sedentary females. J Cosmet Dermatol. 2018.
Lundberg GD. Fat reduction by topical waist applications may actually work. Medscape J Med. 2008;10(2):43. Published 2008 Feb 21.
Available from https://academic.oup.com/asj/article/17/5/304/177651.
Available from https://journals.lww.com/plasreconsurg/fulltext/2013/09000/Thigh_Girth_Loss_in_Women_with_Lower_Body_Fat.61.aspx.
Greenway, F. L., Bray, G. A., & Heber, D. (1995). Topical fat reduction. Obesity research, 3 Suppl 4, 561S–568S. https://doi.org/10.1002/j.1550-8528.1995.tb00228.x.
Escalante, G., Bryan, P., & Rodriguez, J. (2019). Effects of a topical lotion containing aminophylline, caffeine, yohimbe, l-carnitine, and gotu kola on thigh circumference, skinfold thickness, and fat mass in sedentary females. Journal of cosmetic dermatology, 18(4), 1037–1043. https://doi.org/10.1111/jocd.12801.
Caruso, M. K., Roberts, A. T., Bissoon, L., Self, K. S., Guillot, T. S., & Greenway, F. L. (2008). An evaluation of mesotherapy solutions for inducing lipolysis and treating cellulite. Journal of plastic, reconstructive & aesthetic surgery : JPRAS, 61(11), 1321–1324. https://doi.org/10.1016/j.bjps.2007.03.039.
Dickinson, B. I., & Gora-Harper, M. L. (1996). Aminophylline for cellulite removal. The Annals of pharmacotherapy, 30(3), 292–293. https://doi.org/10.1177/106002809603000315.
Available from https://journals.sagepub.com/doi/abs/10.1177/229255039500300409.
Available from https://journals.sagepub.com/doi/abs/10.1177/875512259701300209.
Greenway, F. L., & Bray, G. A. (1987). Regional fat loss from the thigh in obese women after adrenergic modulation. Clinical therapeutics, 9(6), 663–669.
Available from http://www.jarcet.com/articles/Vol14Iss1/Petrofsky3.pdf.
Turan, A., Memiş, D., Karamanlioglu, B., Colak, A., Pamukçu, Z., & Turan, N. (2002). Effect of aminophylline on recovery from sevoflurane anaesthesia. European journal of anaesthesiology, 19(6), 452–454.
El tahan MR. Effects of aminophylline on cognitive recovery after sevoflurane anesthesia. J Anesth. 2011;25(5):648-56.
Turan, A., Memiş, D., Karamanlýodthlu, B., Pamukçu, Z., & Süt, N. (2004). Effect of aminophylline on bispectral index. Acta anaesthesiologica Scandinavica, 48(4), 408–411. https://doi.org/10.1111/j.0001-5172.2004.00350.x.
Furukawa CT, Duhamel TR, Weimer L, Shapiro GG, Pierson WE, Bierman CW. Cognitive and behavioral findings in children taking theophylline. J Allergy Clin Immunol. 1988;81(1):83-8.
Mitrouska I, Kondili E, Prinianakis G, Siafakas N, Georgopoulos D. Effects of theophylline on ventilatory poststimulus potentiation in patients with brain damage. Am J Respir Crit Care Med. 2003;167(8):1124-30.
Alkana, R. L., Parker, E. S., Cohen, H. B., Birch, H., & Noble, E. P. (1977). Reversal of ethanol intoxication in humans: an assessment of the efficacy of L-dopa, aminophylline, and ephedrine. Psychopharmacology, 55(3), 203–212. https://doi.org/10.1007/BF00497849.
Available from https://jptrm.chitkara.edu.in/index.php/jptrm/article/view/13.
Ghaffaripour S, Khosravi MB, Rahimi A, Sahmedini MA, Chohedri A, Mahmoudi H, Kazemi MR. The effects of Aminophylline on clinical recovery and bispectral index in patients anesthetized with total intravenous anaesthesia. Pak J Med Sci. 2014 Nov-Dec;30(6):1351-5. doi: 10.12669/pjms.306.5853. PMID: 25674137; PMCID: PMC4320729.
Kumral, A., Yesilirmak, D. C., Aykan, S., Genc, S., Tugyan, K., Cilaker, S., Akhisaroglu, M., Aksu, I., Sutcuoglu, S., Yilmaz, O., Duman, N., & Ozkan, H. (2010). Protective effects of methylxanthines on hypoxia-induced apoptotic neurodegeneration and long-term cognitive functions in the developing rat brain. Neonatology, 98(2), 128–136. https://doi.org/10.1159/000278840.
Available from https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=521007.
Available from https://www.sid.ir/en/Journal/ViewPaper.aspx?ID=323455.
Available from https://journals.lww.com/ejanaesthesiology/Citation/2001/00001/Aminophylline_speeds_recovery_of_halothane.21.aspx.
Kim, D. W., Joo, J. D., In, J. H., Jeon, Y. S., Jung, H. S., Jeon, K. B., Park, J. S., & Choi, J. W. (2013). Comparison of the recovery and respiratory effects of aminophylline and doxapram following total intravenous anesthesia with propofol and remifentanil. Journal of clinical anesthesia, 25(3), 173–176. https://doi.org/10.1016/j.jclinane.2012.07.005.
Fischer R, Lang SM, Leitl M, Thiere M, Steiner U, Huber RM. Theophylline and acetazolamide reduce sleep-disordered breathing at high altitude. Eur Respir J. 2004;23(1):47-52.
Espinoza H, Antic R, Thornton AT, Mcevoy RD. The effects of aminophylline on sleep and sleep-disordered breathing in patients with obstructive sleep apnea syndrome. Am Rev Respir Dis. 1987;136(1):80-4.
Küpper TE, Strohl KP, Hoefer M, Gieseler U, Netzer CM, Netzer NC. Low-dose theophylline reduces symptoms of acute mountain sickness. J Travel Med. 2008;15(5):307-14.
Raetzo, M. A., Junod, A. F., & Kryger, M. H. (1987). Effect of aminophylline and relief from hypoxia on central sleep apnoea due to medullary damage. Bulletin europeen de physiopathologie respiratoire, 23(2), 171–175.
Louie, G. L., Prokocimer, P. G., Nicholls, E. A., & Maze, M. (1986). Aminophylline shortens thiopental sleep-time and enhances noradrenergic neurotransmission in rats. Brain research, 383(1-2), 377–381. https://doi.org/10.1016/0006-8993(86)90044-2.
Reiterer, F., Schenkeli, R., Kurz, R., & Haidmayer, R. (1988). Effekt einer Aminophyllintherapie beim reifgeborenen Säugling mit Schlafapnoesyndrom [Effect of aminophylline therapy in mature infants with sleep apnea syndrome]. Monatsschrift Kinderheilkunde : Organ der Deutschen Gesellschaft fur Kinderheilkunde, 136(7), 368–371.
- Kuzemko JA, Paala J. Apnoeic attacks in the newborn treated with aminophylline. Arch Dis Child. 1973 May;48(5):404-6. doi: 10.1136/adc.48.5.404. PMID: 4703073; PMCID: PMC1648384.
Rudusky BM. Aminophylline: exploring cardiovascular benefits versus medical malcontent. Angiology. 2005;56(3):295-304.
Matthay RA. Favorable cardiovascular effects of theophylline in COPD. Chest. 1987;92(1 Suppl):22S-26S.
Matthay RA. Effects of theophylline on cardiovascular performance in chronic obstructive pulmonary disease. Chest. 1985;88(2 Suppl):112S-117S.
Vestal RE, Eiriksson CE, Musser B, Ozaki LK, Halter JB. Effect of intravenous aminophylline on plasma levels of catecholamines and related cardiovascular and metabolic responses in man. Circulation. 1983;67(1):162-71.
Walther FJ, Sims ME, Siassi B, Wu PY. Cardiac output changes secondary to theophylline therapy in preterm infants. J Pediatr. 1986;109(5):874-6.
Matthay RA, Mahler DA. Theophylline improves global cardiac function and reduces dyspnea in chronic obstructive lung disease. J Allergy Clin Immunol. 1986;78(4 Pt 2):793-9.
Dutt AK, De soyza ND, Au WY, Hargis JL, Tuck RL. The effect of aminophylline on cardiac rhythm in advanced chronic obstructive pulmonary disease: correlation with serum theophylline levels. Eur J Respir Dis. 1983;64(4):264-70.
Rutherford JD, Vatner SF, Braunwald E. Effects and mechanism of action of aminophylline on cardiac function and regional blood flow distribution in conscious dogs. Circulation. 1981;63(2):378-87.
Mokra D, Tonhajzerova I, Mokry J, Petraskova M, Hutko M, Calkovska A. Cardiovascular side effects of aminophylline in meconium-induced acute lung injury. Adv Exp Med Biol. 2013;756:341-7.
Roig, E., Magriñá, J., Paz, M., Bassa, P., Recasens, L., Huguet, M., Heras, M., & Sanz, G. (1996). Improvement of exercise-induced ischaemia and myocardial perfusion after aminophylline. Coronary artery disease, 7(1), 69–73.
Hempelmann, G., Frerk, C., Piepenbrock, S., & Schleussner, E. (1978). Beeinflussung von Herzkreislaufparametern durch Aminophyllin (Euphyllin) [Cardio-circulatory effects of aminophylline (Euphyllin) (author’s transl)]. Praktische Anasthesie, Wiederbelebung und Intensivtherapie, 13(5), 437–445.
-
Goodfellow, J., & Walker, P. R. (1995). Reversal of atropine-resistant atrioventricular block with intravenous aminophylline in the early phase of inferior wall acute myocardial infarction following treatment with streptokinase. European heart journal, 16(6), 862–865. https://doi.org/10.1093/oxfordjournals.eurheartj.a061008.
Viskin, S., Belhassen, B., Roth, A., Reicher, M., Averbuch, M., Sheps, D., Shalabye, E., & Laniado, S. (1993). Aminophylline for bradyasystolic cardiac arrest refractory to atropine and epinephrine. Annals of internal medicine, 118(4), 279–281. https://doi.org/10.7326/0003-4819-118-4-199302150-00006.
Melville, K. I., & Lu, F. C. (1950). Effect of epinephrine, aminophylline, nitroglycerine and papaverine on coronary inflow and on heart contraction, as recorded concurrently. The Journal of pharmacology and experimental therapeutics, 99(3), 286–303.
Elliott, P. M., Krzyzowska-Dickinson, K., Calvino, R., Hann, C., & Kaski, J. C. (1997). Effect of oral aminophylline in patients with angina and normal coronary arteriograms (cardiac syndrome X). Heart (British Cardiac Society), 77(6), 523–526. https://doi.org/10.1136/hrt.77.6.523
Pasnoori, V. R., & Leesar, M. A. (2004). Use of aminophylline in the treatment of severe symptomatic bradycardia resistant to atropine. Cardiology in review, 12(2), 65–68. https://doi.org/10.1097/01.crd.0000096418.72821.fa.
Whitman, C. B., Schroeder, W. S., Ploch, P. J., & Raghavendran, K. (2008). Efficacy of aminophylline for treatment of recurrent symptomatic bradycardia after spinal cord injury. Pharmacotherapy, 28(1), 131–135. https://doi.org/10.1592/phco.28.1.131.
Murphy, G. W., Schreiner, B. F., Jr, & Yu, P. N. (1968). Effects of aminophylline on the pulmonary circulation and left ventricular performance in patients with valvular heart disease. Circulation, 37(3), 361–369. https://doi.org/10.1161/01.cir.37.3.361.
Huang D, O’brien RG, Harman E, et al. Does aminophylline benefit adults admitted to the hospital for an acute exacerbation of asthma?. Ann Intern Med. 1993;119(12):1155-60.
Mahemuti G, Zhang H, Li J, Tieliwaerdi N, Ren L. Efficacy and side effects of intravenous theophylline in acute asthma: a systematic review and meta-analysis. Drug Des Devel Ther. 2018;12:99-120.
Neame M, Aragon O, Fernandes RM, Sinha I. Salbutamol or aminophylline for acute severe asthma: how to choose which one, when and why?. Arch Dis Child Educ Pract Ed. 2015;100(4):215-22.
Nuhoglu Y, Nuhoglu C. Aminophylline for treating asthma and chronic obstructive pulmonary disease. Expert Rev Respir Med. 2008;2(3):305-13.
Freitag A. Aminophylline injection and theophylline tablets: Acute response in partially reversible chronic airway obstruction. Med J Aust. 1976;1(14):478-9.
- Wrenn K, Slovis CM, Murphy F, Greenberg RS. Aminophylline therapy for acute bronchospastic disease in the emergency room. Ann Intern Med. 1991;115(4):241-7.
Rabe KF, Hiemstra PS. Theophylline for chronic obstructive pulmonary disease?.Time to move on. Am J Respir Crit Care Med. 2010;182(7):868-9.
Shim CS, Williams MH. Bronchodilator response to oral aminophylline and terbutaline versus aerosol albuterol in patients with chronic obstructive pulmonary disease. Am J Med. 1983;75(4):697-701.
Ram FS, Jardin JR, Atallah A, et al. Efficacy of theophylline in people with stable chronic obstructive pulmonary disease: a systematic review and meta-analysis. Respir Med. 2005;99(2):135-44.
Devereux G, Cotton S, Barnes P, et al. Use of low-dose oral theophylline as an adjunct to inhaled corticosteroids in preventing exacerbations of chronic obstructive pulmonary disease: study protocol for a randomised controlled trial. Trials. 2015;16:267. Published 2015 Jun 10. doi:10.1186/s13063-015-0782-2.
Devereux G, Cotton S, Fielding S, et al. Effect of Theophylline as Adjunct to Inhaled Corticosteroids on Exacerbations in Patients With COPD: A Randomized Clinical Trial. JAMA. 2018;320(15):1548-1559.
Luo WJ, Ling X, Huang RM. Effects of aminophylline on cytokines and pulmonary function in patients undergoing valve replacement. Eur J Cardiothorac Surg. 2004;25(5):766-71.
Available from https://www.jacionline.org/article/0091-6749(86)90064-3/fulltext.
Chen CY, Yang KY, Lee YC, Perng PP. Effect of oral aminophylline on pulmonary function improvement and tolerability in different age groups of COPD patients. Chest. 2005;128(4):2088-92.
Barnes PJ. Theophylline in chronic obstructive pulmonary disease: new horizons. Proceedings of the American Thoracic Society. 2005; 2(4):334-9; discussion 340-1.
Chrystyn H, Mulley BA, Peake MD. Dose response relation to oral theophylline in severe chronic obstructive airways disease. BMJ. 1988;297(6662):1506-10.
Georgopoulos D, Holtby SG, Berezanski D, Anthonisen NR. Aminophylline effects on ventilatory response to hypoxia and hyperoxia in normal adults. J Appl Physiol. 1989;67(3):1150-6.
Lim S, Tomita K, Caramori G, et al. Low-dose theophylline reduces eosinophilic inflammation but not exhaled nitric oxide in mild asthma. Am J Respir Crit Care Med. 2001;164(2):273-6.
Sullivan P, Bekir S, Jaffar Z, Page C, Jeffery P, Costello J. Anti-inflammatory effects of low-dose oral theophylline in atopic asthma. Lancet. 1994;343(8904):1006-8.
Parker, J. O., Kelkar, K., & West, R. O. (1966). Hemodynamic effects of aminophylline in cor pulmonale. Circulation, 33(1), 17–25. https://doi.org/10.1161/01.cir.33.1.17.
Fairfax, A. J., McNabb, W. R., Davies, H. J., & Spiro, S. G. (1980). Slow-release oral salbutamol and aminophylline in nocturnal asthma: relation of overnight changes in lung function and plasma drug levels. Thorax, 35(7), 526–530. https://doi.org/10.1136/thx.35.7.526.
Barrett, C. T., Sevanian, A., Phelps, D. L., Gilden, C., & Kaplan, S. A. (1978). Effects of cortisol and aminophylline upon survival, pulmonary mechanics, and secreted phosphatidyl choline of prematurely delivered rabbits. Pediatric research, 12(1), 38–42. https://doi.org/10.1203/00006450-197801000-00010.
Sevanian, A., Gilden, C., Kaplan, S. A., & Barrett, C. T. (1979). Enhancement of fetal lung surfactant production by aminophylline. Pediatric research, 13(12), 1336–1340. https://doi.org/10.1203/00006450-197912000-00007.
Chapman, D. L., Carlton, D. P., Cummings, J. J., Poulain, F. R., & Bland, R. D. (1991). Intrapulmonary terbutaline and aminophylline decrease lung liquid in fetal lambs. Pediatric research, 29(4 Pt 1), 357–361. https://doi.org/10.1203/00006450-199104000-00006.
Gross, I., & Rooney, S. A. (1977). Aminophylline stimulates the incorporation of choline into phospholipid in explants of fetal rat lung in organ culture. Biochimica et biophysica acta, 488(2), 263–269. https://doi.org/10.1016/0005-2760(77)90183-7.
Cosmi, E. V., Saitto, C., Barbati, A., Del Bolgia, F., Di Renzo, G. C., Grossmann, G., Lachmann, B., & Robertson, B. (1986). Effect of aminophylline on lung maturation in preterm rabbit fetuses. American journal of obstetrics and gynecology, 154(2), 436–439. https://doi.org/10.1016/0002-9378(86)90686-1.
Maniscalco, W. M., Wilson, C. M., & Gross, I. (1979). Influence of aminophylline and cyclic AMP on glycogen metabolism in fetal rat lung in organ culture. Pediatric research, 13(12), 1319–1322. https://doi.org/10.1203/00006450-197912000-00003.
Mokra, D., Drgova, A., Mokry, J., Bulikova, J., Pullmann, R., Durdik, P., Petraskova, M., & Calkovska, A. (2008). Combination of budesonide and aminophylline diminished acute lung injury in animal model of meconium aspiration syndrome. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society, 59 Suppl 6, 461–471.
Mokra, D., Mokry, J., Tatarkova, Z., Redfors, B., Petraskova, M., & Calkovska, A. (2007). Aminophylline treatment in meconium-induced acute lung injury in a rabbit model. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society, 58 Suppl 5(Pt 1), 399–407.
Mokra, D., Drgova, A., Mokry, J., Pullmann, R., Redfors, B., Petraskova, M., & Calkovska, A. (2008). Comparison of the effects of low-dose vs. high-dose aminophylline on lung function in experimental meconium aspiration syndrome. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society, 59 Suppl 6, 449–459.
Lindenschmidt, R. C., & Witschi, H. (1985). Attenuation of pulmonary fibrosis in mice by aminophylline. Biochemical pharmacology, 34(24), 4269–4273. https://doi.org/10.1016/0006-2952(85)90283-7.
Wanke, T., Merkle, M., Zifko, U., Formanek, D., Lahrmann, H., Grisold, W., & Zwick, H. (1994). The effect of aminophylline on the force-length characteristics of the diaphragm. American journal of respiratory and critical care medicine, 149(6), 1545–1549. https://doi.org/10.1164/ajrccm.149.6.8004311.
Aubier, M., De Troyer, A., Sampson, M., Macklem, P. T., & Roussos, C. (1981). Aminophylline improves diaphragmatic contractility. The New England journal of medicine, 305(5), 249–252. https://doi.org/10.1056/NEJM198107303050503.
Kennedy, T. P., Michael, J. R., Hoidal, J. R., Hasty, D., Sciuto, A. M., Hopkins, C., Lazar, R., Bysani, G. K., Tolley, E., & Gurtner, G. H. (1989). Dibutyryl cAMP, aminophylline, and beta-adrenergic agonists protect against pulmonary edema caused by phosgene. Journal of applied physiology (Bethesda, Md. : 1985), 67(6), 2542–2552. https://doi.org/10.1152/jappl.1989.67.6.2542.
Mizus, I., Summer, W., Farrukh, I., Michael, J. R., & Gurtner, G. H. (1985). Isoproterenol or aminophylline attenuate pulmonary edema after acid lung injury. The American review of respiratory disease, 131(2), 256–259. https://doi.org/10.1164/arrd.1985.131.2.256.
Sciuto, A. M., Strickland, P. T., Kennedy, T. P., & Gurtner, G. H. (1997). Postexposure treatment with aminophylline protects against phosgene-induced acute lung injury. Experimental lung research, 23(4), 317–332. https://doi.org/10.3109/01902149709039229.
Nowak, D., Rozniecki, J., Ruta, U., Bednarowicz, A., & Izdebski, J. (1988). The influence of aminophylline on human neutrophils–possible protection of lung from proteolytic injury. Archivum immunologiae et therapiae experimentalis, 36(3), 351–360.
Mitra, A., Bassler, D., Goodman, K., Lasserson, T. J., & Ducharme, F. M. (2005). Intravenous aminophylline for acute severe asthma in children over two years receiving inhaled bronchodilators. The Cochrane database of systematic reviews, 2005(2), CD001276. https://doi.org/10.1002/14651858.CD001276.pub2.
Protective Effect of Aminophylline against Cigarette Smoke Extract–Induced Apoptosis in Human Lung Fibroblasts (MRC-5 Cells).
Armanian AM, Badiee Z, Afghari R, Salehimehr N, Hassanzade A, Sheikhzadeh S, Shariftehrani M, Rezvan G. Reducing the incidence of chronic lung disease in very premature infants with aminophylline. Int J Prev Med. 2014 May;5(5):569-76. PMID: 24932388; PMCID: PMC4050677.
Hadjigeorgiou, E., Kitsiou, S., Psaroudakis, A., Segos, C., Nicolopoulos, D., & Kaskarelis, D. (1979). Antepartum aminophylline treatment for prevention of the respiratory distress syndrome in premature infants. American journal of obstetrics and gynecology, 135(2), 257–260. https://doi.org/10.1016/0002-9378(79)90355-7.
Axelrod DM, Anglemyer AT, Sherman-levine SF, et al. Initial experience using aminophylline to improve renal dysfunction in the pediatric cardiovascular ICU. PediatrCrit Care Med. 2014;15(1):21-7.
Bhatt GC, Gogia P, Bitzan M, Das RR. Theophylline and aminophylline for prevention of acute kidney injury in neonates and children: a systematic review. Arch Dis Child. 2019.
Djaladat H, Tajik P, Fard SA, Alehashemi S. The effect of aminophylline on renal colic: a randomized double blind controlled trial. South Med J. 2007;100(11):1081-4.
Mcmahon K, Zappitelli M. Aminophylline for Acute Kidney Injury After Pediatric Cardiac Surgery: Finally Entering the Next Phase in Child Acute Kidney Injury Research. PediatrCrit Care Med. 2016;17(2):170-1.
Lynch BA, Gal P, Ransom JL, et al. Low-dose aminophylline for the treatment of neonatal non-oliguric renal failure-case series and review of the literature. J PediatrPharmacolTher. 2008;13(2):80–87. doi:10.5863/1551-6776-13.2.80.
Mazkereth R, Laufer J, Jordan S, Pomerance JJ, Boichis H, Reichman B. Effects of theophylline on renal function in premature infants. Am J Perinatol. 1997;14(1):45-9.
Mccullough PA, Larsen T, Brown JR. Theophylline or aminophylline for the prevention of contrast-induced acute kidney injury. Am J Kidney Dis. 2012;60(3):338-9.
Ix JH, Mcculloch CE, Chertow GM. Theophylline for the prevention of radiocontrast nephropathy: a meta-analysis. Nephrol Dial Transplant. 2004;19(11):2747-53.
Available from https://clinicaltrials.gov/ct2/show/NCT02983422.
Parker MR, Willatts SM. A pilot study to investigate the effects of an infusion of aminophylline on renal function following major abdominal surgery. Anaesthesia. 2001;56(7):670-5.
Benoehr P, Krueth P, Bokemeyer C, Grenz A, Osswald H, Hartmann JT. Nephroprotection by theophylline in patients with cisplatin chemotherapy: a randomized, single-blinded, placebo-controlled trial. J Am Soc Nephrol. 2005;16(2):452-8.
Abizaid, A. S., Clark, C. E., Mintz, G. S., Dosa, S., Popma, J. J., Pichard, A. D., Satler, L. F., Harvey, M., Kent, K. M., & Leon, M. B. (1999). Effects of dopamine and aminophylline on contrast-induced acute renal failure after coronary angioplasty in patients with preexisting renal insufficiency. The American journal of cardiology, 83(2), 260–A5. https://doi.org/10.1016/s0002-9149(98)00833-9.
Barzegarnezhad, A., Firouzian, A., Emadi, S. A., Mousanejad, N., & Bakhshali, R. (2012). The effects of local administration of aminophylline on transureteral lithotripsy. Advances in urology, 2012, 727843. https://doi.org/10.1155/2012/727843.
Seo, K., Choi, J. W., Kim, D. W., Han, D., Noh, S. J., & Jung, H. S. (2017). Aminophylline Effect on Renal Ischemia-Reperfusion Injury in Mice. Transplantation proceedings, 49(2), 358–365. https://doi.org/10.1016/j.transproceed.2016.11.043.
Available from https://www.kireports.org/article/S2468-0249(22)00047-X/fulltext.
Sauer HE, Crews KR, Pauley JL, Bourque MS, Bragg AW, Triplett B, Morrison RR, Hall EA. Evaluation of Aminophylline for the Treatment of Acute Kidney Injury in Pediatric Hematology/Oncology Patients. J Pediatr Pharmacol Ther. 2021;26(5):484-490. doi: 10.5863/1551-6776-26.5.484. Epub 2021 Jun 28. PMID: 34239401; PMCID: PMC8244958.
Alsaadoun S, Rustom F, Hassan HA, Alkhurais H, Aloufi M, Alzahrani S, Bakhsh S, Dalbhi SA. Aminophylline for improving acute kidney injury in pediatric patients: A systematic review and meta-analysis. Int J Health Sci (Qassim). 2020 Nov-Dec;14(6):44-51. PMID: 33192231; PMCID: PMC7644458.
Available from https://journals.lww.com/pccmjournal/Citation/2016/08000/Use_of_Aminophylline_to_Prevent_Acute_Kidney.26.aspx.
Bellos, I., Iliopoulos, D. C., & Perrea, D. N. (2019). Pharmacological interventions for the prevention of acute kidney injury after pediatric cardiac surgery: a network meta-analysis. Clinical and experimental nephrology, 23(6), 782–791. https://doi.org/10.1007/s10157-019-01706-9.
Van den Eynde, J., Cloet, N., Van Lerberghe, R., Sá, M., Vlasselaers, D., Toelen, J., Verbakel, J. Y., Budts, W., Gewillig, M., Kutty, S., Pottel, H., & Mekahli, D. (2021). Strategies to Prevent Acute Kidney Injury after Pediatric Cardiac Surgery: A Network Meta-Analysis. Clinical journal of the American Society of Nephrology : CJASN, 16(10), 1480–1490. https://doi.org/10.2215/CJN.05800421.
Leow, E. H., Chan, Y. H., Ng, Y. H., Lim, J., Nakao, M., & Lee, J. H. (2018). Prevention of Acute Kidney Injury in Children Undergoing Cardiac Surgery: A Narrative Review. World journal for pediatric & congenital heart surgery, 9(1), 79–90. https://doi.org/10.1177/2150135117743211.
Onder AM, Rosen D, Mullett C, Cottrell L, Kanosky S, Grossman OK, Iqbal HI, Seachrist E, Samsell L, Gustafson K, Rhodes L, Gustafson R. Comparison of Intraoperative Aminophylline Versus Furosemide in Treatment of Oliguria During Pediatric Cardiac Surgery. Pediatr Crit Care Med. 2016 Aug;17(8):753-63. doi: 10.1097/PCC.0000000000000834. PMID: 27355823; PMCID: PMC5515381.
Axelrod DM, Sutherland SM, Anglemyer A, Grimm PC, Roth SJ. A Double-Blinded, Randomized, Placebo-Controlled Clinical Trial of Aminophylline to Prevent Acute Kidney Injury in Children Following Congenital Heart Surgery With Cardiopulmonary Bypass. Pediatr Crit Care Med. 2016 Feb;17(2):135-43. doi: 10.1097/PCC.0000000000000612. PMID: 26669642; PMCID: PMC4740222.
Saboute, M., Balasi, J., Tajalli, S., Hajipour, M., Heshmat, S., Khalesi, N., & Allahqoli, L. (2020). Effect of Aminophylline in Preventing Renal Dysfunction among Neonates with Prenatal Asphyxia: A Clinical Trial. Archives of Iranian medicine, 23(5), 312–318. https://doi.org/10.34172/aim.2020.20.
Available from https://ijp.mums.ac.ir/article_19738.html.
Chock, V. Y., Cho, S. H., & Frymoyer, A. (2021). Aminophylline for renal protection in neonatal hypoxic-ischemic encephalopathy in the era of therapeutic hypothermia. Pediatric research, 89(4), 974–980. https://doi.org/10.1038/s41390-020-0999-y.
Available from https://link.springer.com/article/10.1007/s00431-021-04128-6.
Kinbara, T., Hayano, T., Ohtani, N., Furutani, Y., Moritani, K., & Matsuzaki, M. (2010). Efficacy of N-acetylcysteine and aminophylline in preventing contrast-induced nephropathy. Journal of cardiology, 55(2), 174–179. https://doi.org/10.1016/j.jjcc.2009.10.006.
Milani, L., Merkel, C., & Gatta, A. (1983). Renal effects of aminophylline in hepatic cirrhosis. European journal of clinical pharmacology, 24(6), 757–760. https://doi.org/10.1007/BF00607083.
- Available from https://scumj.journals.ekb.eg/article_54222.html.
Heidemann HT, Müller S, Mertins L, Stepan G, Hoffmann K, Ohnhaus EE. Effect of aminophylline on cisplatin nephrotoxicity in the rat. Br J Pharmacol. 1989 Jun;97(2):313-8. doi: 10.1111/j.1476-5381.1989.tb11956.x. PMID: 2758217; PMCID: PMC1854525.
Rangel, M. O., Morales Demori, R., Voll, S. T., Wassouf, M., Dick, R., & Doukky, R. (2015). Severe chronic kidney disease as a predictor of benefit from aminophylline administration in patients undergoing regadenoson stress myocardial perfusion imaging: A substudy of the ASSUAGE and ASSUAGE-CKD trials. Journal of nuclear cardiology : official publication of the American Society of Nuclear Cardiology, 22(5), 1008–1018. https://doi.org/10.1007/s12350-014-0036-9.
Doukky, R., Rangel, M. O., Dick, R., Wassouf, M., Alqaid, A., & Margeta, B. (2013). Attenuation of the side effect profile of regadenoson: a randomized double-blind placebo-controlled study with aminophylline in patients undergoing myocardial perfusion imaging and have severe chronic kidney disease–the ASSUAGE-CKD trial. The international journal of cardiovascular imaging, 29(5), 1029–1037. https://doi.org/10.1007/s10554-012-0166-6.
Olowu, W. A., & Adefehinti, O. (2012). Aminophylline improves urine flow rates but not survival in childhood oliguric/anuric acute kidney injury. Arab journal of nephrology and transplantation, 5(1), 35–39.
Mahaldar AR, Sampathkumar K, Raghuram AR, Kumar S, Ramakrishnan M, Mahaldar DA. Risk prediction of acute kidney injury in cardiac surgery and prevention using aminophylline. Indian J Nephrol. 2012 May;22(3):179-83. doi: 10.4103/0971-4065.98752. PMID: 23087551; PMCID: PMC3459520.
Shahbazi S, Alishahi P, Asadpour E. Evaluation of the Effect of Aminophylline in Reducing the Incidence of Acute Kidney Injury After Cardiac Surgery. Anesth Pain Med. 2017 Aug 27;7(4):e21740. doi: 10.5812/aapm.21740. PMID: 29696106; PMCID: PMC5903222.
Success Stories
 before after
before after
At the age of 60, I look and feel better than I ever have in my entire life! Switching my health program and hormone replacement therapy regimen over to Genemedics was one of the best decisions I’ve ever made in my life! Genemedics and Dr George have significantly improved my quality of life and also dramatically improved my overall health. I hav...
Nick Cassavetes ,60 yrs old
Movie Director (“The Notebook”, “John Q”, “Alpha Dog”), Actor and Writer

Call 800-277-4041 for a Free Consultation
- Usually takes 15-30 minutes
- Completely confidential
- No obligation to purchase anything
- We will discuss your symptoms along with your health and fitness goals
- Free post-consult access for any additional questions you may have
© Copyright Genemedics Health Institute. All Rights Reserved. Privacy Policy.